PCOS
Read Time: 6min
Written By

Dr. Hassan Khan
Internist
PCOS Explained: What Is Polycystic Ovary Syndrome?
PCOS (Polycystic Ovary Syndrome) is a common hormone condition that can affect your period, skin, hair growth, metabolism, and fertility. However, it’s often misunderstood—and many people go years without a clear diagnosis. The good news is that PCOS is manageable with the right plan and follow-up care.
Table of Contents
FAQs
PCOS FAQs
Please feel free to Send a Message or call us if your related question is not included here. we are happy to serve you.
Not necessarily. The name is misleading. Many people have follicles on ultrasound. PCOS is more about hormone patterns and ovulation.
Yes. PCOS can occur at any body size. Symptoms and hormone patterns matter more than weight alone.
PCOS is usually long-term. However, symptoms can improve a lot with treatment and consistent follow-up.
PCOS is a common cause of infertility, mainly because it can disrupt ovulation.
Evidence-based guidance supports letrozole as a first-line ovulation induction option for many women with PCOS.
If you have irregular periods, signs of high androgens (acne, unwanted hair), or fertility concerns, it’s worth getting evaluated.
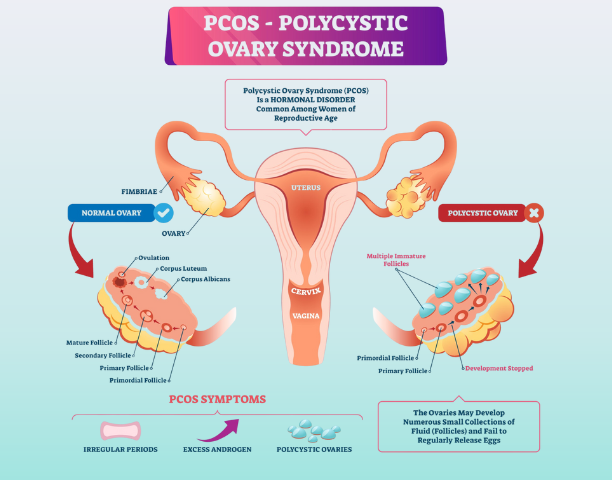
What Is Polycystic Ovary Syndrome (PCOS)?
PCOS stands for polycystic ovary syndrome. It’s a hormone-related condition that may involve irregular ovulation, higher androgen levels (androgens are hormones like testosterone), and/or a specific appearance of the ovaries on ultrasound.
Important: PCOS does not mean your ovaries are “full of cysts.” The term “polycystic” can be confusing because many people with PCOS have follicles (immature eggs) that do not mature and ovulate regularly. In other words, it’s mainly about ovulation and hormone patterns, not dangerous cysts.
PCOS is common worldwide. The World Health Organization notes PCOS affects a meaningful share of reproductive-age women and can affect both physical and mental health.
Polycystic Ovary Syndrome Symptoms (What You May Notice)
PCOS symptoms vary. Some people have clear signs early. Others have subtle symptoms for years.
Common Polycystic Ovary Syndrome symptoms include:
- Irregular periods (long cycles, missed periods, unpredictable bleeding)
- Acne or oily skin that persists past the teen years
- Unwanted hair growth on face/chest/abdomen (hirsutism)
- Hair thinning on the scalp
- Weight gain or difficulty losing weight (not everyone)
- Fertility challenges due to irregular ovulation
- Darkened skin patches (sometimes)
Also, mental health matters. WHO notes PCOS can be associated with anxiety, depression, and negative body image.
What Causes Polycystic Ovary Syndrome?
There is no single cause. Instead, Polycystic Ovary Syndrome is usually a mix of genetics, hormone signaling, and metabolic factors.
Here are common drivers clinicians consider:
Insulin resistance (common in PCOS)
Many people with Polycystic Ovary Syndrome have insulin resistance. That can raise insulin levels, which can influence androgen production and ovulation patterns.
Higher androgen levels
Androgens are normal in all bodies. However, higher levels may contribute to acne, unwanted hair growth, and disrupted ovulation.
Genetics and family history
PCOS tends to run in families. That suggests a genetic component, even though there isn’t one “PCOS gene.”
Inflammation and lifestyle pressures
Stress, sleep problems, and weight changes can worsen symptoms. So PCOS care often includes lifestyle support as part of the medical plan.
How PCOS Is Diagnosed (Rotterdam Criteria)
A PCOS diagnosis should feel structured, not random.
Many clinicians use the Rotterdam criteria, which generally require two out of three features (after ruling out other causes):
- Irregular or absent ovulation
- Clinical or lab signs of hyperandrogenism
- Polycystic ovarian morphology on ultrasound
Why “ruling out other causes” is important
PCOS symptoms can overlap with thyroid disorders, high prolactin, adrenal conditions, and other hormone issues. So a good evaluation checks for common look-alikes.
PCOS diagnosis can differ in teens
In adolescents, ultrasound can be less helpful because ovarian appearance can look “polycystic” even in normal puberty. That’s why many guidelines emphasize careful diagnosis in teens.
PCOS and Infertility (Why Ovulation Matters)
PCOS is one of the most common causes of infertility because it can prevent regular ovulation.
If you don’t ovulate regularly, timing intercourse becomes difficult and pregnancy becomes less likely each month. However, many people with PCOS do conceive. The path is often clearer once ovulation is addressed.
What “ovulation induction” means
Ovulation induction is medical support to help the body release an egg more consistently.
Evidence-based guidance supports letrozole as a first-line ovulation induction medication for many women with PCOS because it improves ovulation and live birth outcomes compared with some older options.
Treatment Options (What Actually Helps)
There isn’t a single “best” PCOS plan. Instead, treatment depends on your main goal: symptom control, cycle regulation, fertility, or metabolic health.
Treatment for irregular periods
Cycle regulation can reduce unpredictable bleeding and support uterine health. Options may include hormonal approaches discussed with your clinician, based on your medical history and goals.
Treatment for acne and unwanted hair
Androgen-related symptoms often improve with medical strategies and time. Also, skincare and hair management can be part of the plan, especially when symptoms affect confidence.
Treatment for metabolic health and weight
Lifestyle changes are not “basic advice.” They are a clinical tool. Even modest weight loss can improve cycles and ovulation for some patients.
Try this practical structure:
- Protein-forward breakfasts
- Daily fiber target (vegetables + legumes + whole foods)
- 2–3 strength sessions weekly (even short)
- Consistent sleep window (same wake time most days)
PCOS infertility treatment (ovulation support)
If pregnancy is the goal, your clinician may focus on ovulation induction and timing strategies. Letrozole is commonly recommended as first-line in evidence-based guidance for PCOS-related infertility.
Mental health support is part of PCOS care.
It can impact mood, self-image, and stress. WHO highlights mental health effects as part of the condition’s burden.
If you feel dismissed, it’s reasonable to ask for care that takes both physical and emotional symptoms seriously.
Long-Term Health Risks and Complications
PCOS is not only about periods or fertility.
It can be associated with:
- Higher risk of type 2 diabetes and metabolic issues
- High blood pressure and cholesterol concerns
- Endometrial hyperplasia/cancer risk if prolonged irregular shedding occurs
- Sleep issues and obstructive sleep apnea in some patients
That sounds heavy. However, it’s also empowering—because monitoring and prevention can make a real difference.
Practical Checklist (Getting the Most From a Polycystic Ovary Syndrome Appointment)
Bring clarity to your visit. This helps you get answers faster.
Symptom tracking
- Cycle dates for the last 3–6 months
- Acne/hair changes timeline
- Weight changes and appetite patterns
- Sleep quality and stress level
Questions to ask your clinician
- “Do my symptoms fit PCOS or something else?”
- “Which labs do I need, and why?”
- “Am I ovulating regularly?”
- “If I want pregnancy, what is our step-by-step plan?”
- “How will we follow up and track progress?”
Red flags to mention right away
- Heavy bleeding that soaks pads hourly
- Severe pelvic pain
- Rapid hair loss or sudden high-androgen symptoms
- Depression or anxiety that feels unmanageable
Mini Case Example (What PCOS Can Look Like)
Case: A 26-year-old has irregular periods (every 45–70 days), acne that worsened after college, and new chin hair. She also feels exhausted and has sugar cravings.
What changed her care:
First, her clinician confirmed she was not ovulating regularly. Next, basic labs ruled out common look-alikes. Then, the plan focused on two lanes: cycle regulation + metabolic support. Within months, cycles became more predictable, acne improved, and her energy stabilized. Later, when she wanted pregnancy, her plan shifted to ovulation induction support.
This is the goal: a plan that matches your life stage.
This article was reviewed and written with insights from the medical team at MindShape Clinic in the USA — experienced healthcare professionals specializing in cancer treatment, mental health, and patient wellness. Learn more about our board-certified doctors and treatment experts who contribute to our educational blogs and patient support programs.
Recent Blogs
Learn more about Virtual Healthcare and Treatments






Why You Can Rely on Us?
At Mindshape Clinic, we are committed to providing clear and trustworthy health information that you can rely on.
Reliable Information – Every article is based on credible sources.
Expert Review – Content is carefully checked before publishing.
Up to Date – We keep information current with the latest insights.
Clarity First – Our goal is to make knowledge simple and accessible.